

Translate this page into:
Effectiveness of Basic Life Support Training Program on Knowledge, Attitude, and Self-Efficacy in Management of Drowning Among Adults Living in Coastal Areas of Mangaluru
Address for correspondence Leena K. Chacko, PhD, Msc, Department of Community Health NursingYenepoya Nursing College, Yenepoya (deemed to be) University, Deralakatte, Mangaluru, Karnataka, India (e-mail: leenakchacko@gmail.com).
This article was originally published by Thieme Medical and Scientific Publishers Pvt. Ltd. and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Introduction
Drowning is a major, but often neglected, public health problem in India. About 97% of all deaths from drowning occur in low- and middle-income countries. Drowning is a preventable morbidity and mortality worldwide. Early use of basic life support (BLS) by a rescuer on site is crucial for the survival of victims of drowning.
Aim
This article aims to find out the effectiveness of BLS training program on knowledge, attitude, and self-efficacy in the management of drowning.
Materials and Methods
A preexperimental, one-group pretest, posttest study design was adopted to study 91 purposively selected subjects who met the selection criteria. The sample size was estimated using a research article by Joseph et al. The data were collected by using valid and reliable tools: 25-item knowledge questionnaire (r = 0.846), 15-item attitude scale (r = 0.867), and 12-item self-efficacy scale (r = 0.928). Ethical approval and informed consent obtained. After obtaining baseline data, pretest was conducted using the said tools and BLS training in the management of drowning was provided. Posttest assessment of knowledge, attitude, and self-efficacy was done 7 days after intervention.
Results
More than three-fourths (80.2%) had inadequate knowledge during pretest, whereas in posttest half (49.5%) had adequate level of knowledge, with mean and standard deviation of 11.18 ± 3.82 in pretest and 18.21 ± 3.08 in posttest. Regarding attitude, more than half (63.7%) had neutral attitude during pretest and three-fourths (73.6%) had positive attitude in posttest with mean and standard deviation of 57.38 ± 6.44 in pretest and 64.87 ± 5.10 in posttest. A poor level of self-efficacy was reported among 58.2% in pretest, whereas 59.3% had fair level of self-efficacy in posttest. Mean and standard deviation was found to be 33.48 ± 7.73 in pretest and 46.25 ± 4.35 in posttest. There was a significant difference in the pretest and posttest scores of knowledge, attitude, and self-efficacy toward BLS at p < 0.05, indicating that BLS training is effective. The Karl Pearson correlation coefficient test showed a significant correlation between knowledge-attitude (r = 0.628, p < 0.001), knowl-edge-self-efficacy (r = 0.820, p < 0.001), and attitude-self efficacy (r = 0.616, p < 0.001).
Conclusion
This study concluded that the BLS training program is effective on knowledge, attitude, and self-efficacy in the management of drowning.
Keywords
BLS and CPR
adult
training
first aid

Introduction
Drowning is the process of experiencing respiratory impairment from submersion/immersion in liquid.1 An estimated 236,000 people died from drowning, making drowning a major public health problem worldwide, and injuries accounted for almost 8% of total global mortality. Drowning is the third leading cause of unintentional death, accounting for 7% of all injury-related deaths.2 And according to the World Health Organization, 0.7% of all deaths worldwide (> 500,000 deaths) annually are attributed to unintentional drowning. About 97% of all deaths from drowning occur in low- and middle-income countries (LMICS).3 The rate of drowning is 82 cases per day in India.4 Karnataka (2,486 or 8%) contributes significantly to the national drowning toll, highlighting the need for increased awareness, preventive measures, and improved water safety programs in the region.5 Drowning is to blame for significant preventable morbidity and mortality worldwide causing more deaths than war.6 In LMICs, drowning often occurs as a result of the activities related to daily life,7 whereas the recreational undertakings often being conducted before drowning in high-income countries (HICs).8
South Asian countries have higher death rates by drowning compared to the globe average. Among drowning survivors, approximately 69% have complete neurological recovery, 28% suffer some selective deficit, and 3% survive to live in a permanent vegetative state. According to the National Crime Records Bureau-Accidental Deaths and Suicides, 80 persons die of drowning daily in India, which accounts for 7.4% of all unnatural deaths. Studies estimated that in 2013 there have been 29,456 deaths by drowning and 440 deaths due to malaria.9
The explanation for drowning is multifactorial and varies with age and geography. It is common in coastal areas mainly due to fishing and swimming activities. It happens mostly in places that have tourist attraction spots near the ocean. Children, males and individuals with increased access to water are most in danger of drowning. Tourists are a high-risk group for drowning.10 They are generally unacquainted with the beach and its safety measures and have poor knowledge of beach hazards like rip currents and breaking waves. This lack of data is further exacerbated by language barriers, overconfidence swimming ability, and therefore the tendency to create unwise swimming decisions after too many beers and umbrella drinks. Interventions at supported site-specific locations are likely to possess a greater impact and prove more successful than general strategies aimed toward drowning prevention.11
Basic life support (BLS) is a vital component of cardiopulmonary resuscitation (CPR), which incorporates adequate maintenance of ventilation and circulation in case of respiratory or cardiac arrest. BLS may be a level of treatment that is offered to victims of life-threatening illness or injuries until they seek full treatment at a hospital.12 The lack of information among the general public regarding the performance of Basic Life Support (BLS) has been a significant issue. Life-saving interventions are crucial for the chain of survival, as they help reduce the impact of sudden medical emergencies.13
CPR provided by BLS-trained primary care providers and community-first responders plays a vital role in prevention. It is estimated that more than 85% of drowning cases could be prevented with supervision, swimming instruction, technology, regulation, and public education. Less than 6% of all persons who are rescued by lifeguards need medical attention in the hospital. Education is fundamental to preventing drowning accidents.14 Therefore, to reduce the number of casualties, BLS/CPR is a critical component of emergency treatment. Unlike in developed countries, where laypersons are the first responders equipped with BLS/CPR skills, in India, these services are mostly provided by a limited number of healthcare professionals. The novelty of this study lies in preparing the local community to save lives, which represents the future of BLS implementation. Out-of-hospital cardiac arrest is the leading cause of death worldwide. Performing BLS immediately can decrease the mortality rate. The need of this study was to compare the knowledge, attitude, and self-efficacy regarding BLS in the management of drowning before and after participating in a BLS training program. Additionally, the study aimed to evaluate the effectiveness of BLS training program in the management of drowning, with the goal of increasing the number of rescuers among adults living in coastal areas of Mangaluru.
Material and Methods
A preexperimental, one-group pretest, posttest study design was adopted in the study. The investigator being a male, the area being at the beachside where male members frequent, and anticipating cultural restrictions for women, the study was conducted among 91 adult males living in coastal areas of Mangaluru, Karnataka, India. The study setting was at the youth club of the Ullal Beach area 2 to 3 km from Ullal taluka headquarters, Dakshina Kannada district where a population of 53,808 live. The subjects were recruited using a nonprobability purposive sampling technique. The study included adult males who are at the age of 18 to 45 years, living in coastal areas of Mangaluru, and able to read and write Kannada. Adults who were with physical disabilities that make them incapable of performing chest compression and any alteration in sensory perception were excluded. The sample size was computed using a reference research article published by Joseph et al in the year 2011.15 To calculate the sample size with a 95% confidence level, a standard normal score Z = 1.96, an anticipated proportion p = 56%, and a margin of error e = 10%, use the formula: which gives a total estimated sample size of 91.
Data Collection Tools
The tools for the data collection were structured knowledge questionnaire and Likert scales for attitude and self-efficacy. The content validity was established by nine experts with their valuable suggestions and recommendations. The tool was modified according to expert suggestions. The tool was pretested by administering in 10 samples. It was found to be clear and feasible.
The structured knowledge questionnaire contained 25 items related to BLS in the management of drowning. Scoring key was designed where each correct answer was awarded 1 mark and the wrong answer 0. Thus, the item maximum score is 25 and the minimum is 0. Knowledge scores of above 19 to 25% or 60 to > 80% were considered “adequate,” knowledge scores of 14 to 18% or 40 to 60% were considered “moderate,” and knowledge scores of below 13 or < 40% were considered as “inadequate” knowledge. The scoring was adopted based on the previous study.16 The reliability of structured knowledge questionnaire was computed by split-half method and Spearman-Brown prophecy formula. Coefficient of correlation of knowledge test was found to be r = 0.846.
The attitude was assessed by using 5-point Likert scale for attitude containing 15 items. The responses were five levels ranging from 1 (strongly disagree) to 5 (strongly agree), respectively. The maximum score is 75 and minimum score is 15. Attitude scores of 61 to 75 were considered “positive,” attitude scores of 46 to 60 were considered “neutral,” and attitude scores of 15 to 45 were considered as “negative” attitude. The reliability of internal consistency for attitude scale was established using Cronbach's alpha coefficient, r = 0.867.
Likert scale for self-efficacy consists of 12 items toward BLS in the management of drowning. Responses were five levels ranging from 1 (not at all true) to 5 (exactly true) Thus, the item's maximum score is 60 and the minimum is 12. Selfefficacy scores of above 49 to 60 were considered “good,” self-efficacy scores of 37 to 48 were considered “fair,” and self-efficacy scores of 12 to 36 were considered as “poor.” The reliability measure of internal consistency was Cronbach's alpha coefficient, r = 0.928. The pilot study was conducted with 10 samples to know the feasibility. No changes were made after the pilot study.
Data collection procedure: Approval for the study was obtained from the institutional ethics committee. Through informal community leaders and youth of the area subjects who meet the selection criteria and willing to take part in the study were identified. After self-introduction, the researcher explained the purpose of the study and obtained written informed consent from each subject and they were assured confidentiality. Sessions were handled in three small groups with the help of three research assistants who were BLS- and ACLS-certified registered nurses, associated with the advanced simulation center as trainers, who were trained further by the researcher about the research expectations. Standardization of procedure skills and assessments were done in the central advanced simulation center of the university, which is an American Heart Association (AHA) certified center. On day 1, after obtaining baseline data, pretest was conducted to assess knowledge, attitude, and self-efficacy toward BLS training. It took an average of about 40 minutes to respond to the tools. On the second day, the investigator took the training session for about 45 to 50 minutes to explain the basics of resuscitation using PowerPoint, videos, and discussion. On the third day, the BLS training intervention was planned and necessary equipment borrowed from the simulation center were setup. Subjects were arranged in groups of 15, and at three adjacent stations the skills were demonstrated. Practices by the subjects were ensured by setting up 15 more mannequins, and once they felt comfortable, a return demonstration was obtained from each participant. All the mannequins had sensors to indicate correctness of the compressions. This took about 45 to 50 minutes per person. As was the pretest, posttest for the assessment of knowledge, attitude, and selfefficacy was done on the 7th day after the intervention by administering structured tools wherein subjects responded by tick marking the responses.
Results
Demographic Characteristics
The present study reveals that more than one-fourth (38.5%) of the age group belonged to 26 to 35 years, 45.1% had plus two levels of education, and 64.8% had below poverty line level of family economic status. Note that 29.7% of the adults were self-employed and were having fishing-related work. More than three-fourths (97.8%) of the adults had not attended any BLS training in the past and none of the adults had resuscitated anyone in the past (Figs. 1–3).

- Adults according to the pretest and posttest knowledge scores in the management of drowning. The figure shows that three-fourths (80.2%) of the adults had inadequate level of knowledge during pretest and 49.5% adequate level of knowledge found in posttest regarding basic life support in the management of drowning.
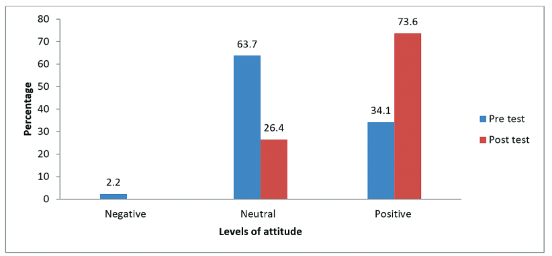
- Adults according to the pretest and posttest attitude scores in the management of drowning. The figure shows that three-fourths (63.7%) of the adults had neutral attitude during pretest and 73.6% positive attitude found in posttest regarding basic life support in the management of drowning.
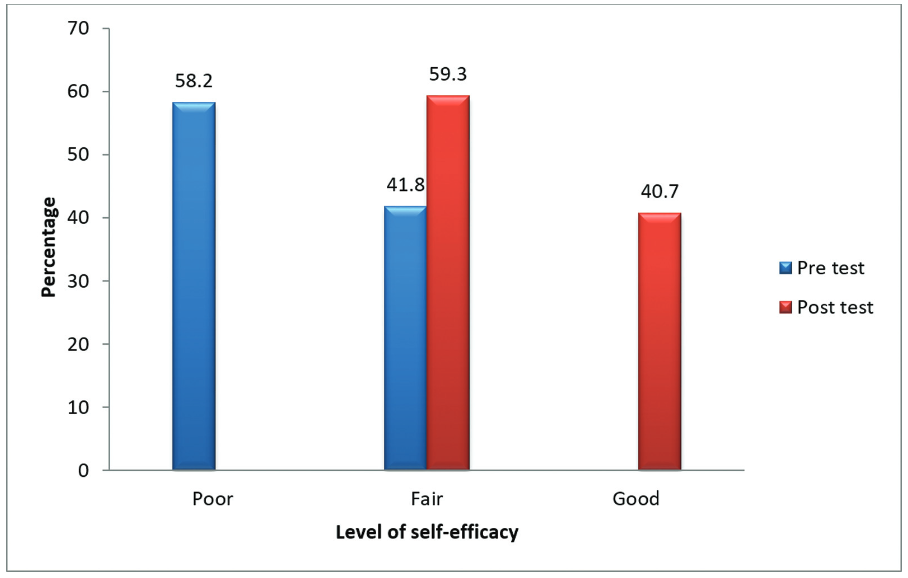
- Adults according to the pretest and posttest self-efficacy scores in the management of drowning. This figure shows that more than half (58.2%) of the adults had poor self-efficacy during pretest but fair self-efficacy (59.3%) found in posttest regarding basic life support in the management of drowning.
Table 1 shows that more than three-fourths (80.2%) of the adults had inadequate level of knowledge during pretest and 49.5% had adequate level of knowledge. More than half (63.7%) had neutral attitude during pretest but three-fourths (73.6%) of the adults showed positive attitude in posttest. More than half (58.2%) of the adults had poor self-efficacy during pretest but more than half (59.3%) of the adults showed fair self-efficacy in posttest regarding BLS in the management of drowning.
| N =91 | ||||||
|---|---|---|---|---|---|---|
| Serial no. | Parameters | Scoring | Pretest | Posttest | ||
| 1. | Level of knowledge | f (%) | Mean ± SD | f (%) | Mean ± SD | |
| Inadequate | 0–13 | 73 (80.2) | 11.18 ± 3.82 | 4 (4.4) | 18.21 ± 3.08 | |
| Moderate | 14–18 | 16 (17.6) | 42 (46.1) | |||
| Adequate | 19–25 | 2 (2.2) | 45 (49.5) | |||
| 2. | Level of attitude | |||||
| Negative | 15–45 | 2 (2.2) | 57.38 ± 6.44 | – | 64.87 ± 5.10 | |
| Neutral | 46–60 | 58 (63.7) | 24 (26.4) | |||
| Positive | 61–75 | 31 (34.1) | 67 (73.6) | |||
| 3. | Self-efficacy | |||||
| Poor | 12–36 | 53 (58.2) | 33.48 ± 7.73 | – | 46.25 ± 4.35 | |
| Fair | 37–48 | 38 (41.8) | 54 (59.3) | |||
| Good | 49–60 | – | 37 (40.7) | |||
Abbreviations: f, frequency; SD, standard deviation.
Table 2 showed that paired t-test was used to test the effectiveness of BLS training on knowledge, attitude, and selfefficacy of subjects in BLS in the management of drowning. Mean pretest (11.18 ± 3.82) and mean posttest (18.21 ± 3.08) knowledge scores indicate a significant increase in knowledge (p < 0.001**). Mean attitude of pretest (57.38 ± 6.44) to mean attitude of posttest (64.87 ± 5.10) showed a significant improvement in attitude scores after BLS training, indicating statistical significance (p < 0.001**). Mean self-efficacy scores of pretest (33.48 ± 7.73) to mean self-efficacy score of posttest (46.25 ±4.35) also showed a significant improvement following BLS training (p = 0.001 **). The results suggest that BLS training had a substantial positive impact on participants' knowledge, attitude, and self-efficacy regarding the management of drowning incidents.
| N =91 | |||||
|---|---|---|---|---|---|
| Variables | Time | Mean ± SD | Mean difference | t-Value | p-Value |
| Knowledge | Pretest | 11.18 ± 3.82 | 7.03 | 30.175 | 0.001a |
| Posttest | 18.21 ± 3.08 | ||||
| Attitude | Pretest | 57.38 ± 6.44 | 7.48 | 20.105 | 0.001a |
| Posttest | 64.87 ± 5.10 | ||||
| Self-efficacy | Pretest | 33.48 ± 7.73 | 12.77 | 27.343 | 0.001a |
| Posttest | 46.25 ± 4.35 | ||||
Abbreviations: BLS, basic life support; SD, standard deviation.
The Karl Pearson correlation coefficient test was computed to assess the correlation between the knowledge and attitude, knowledge and self-efficacy, and attitude and selfefficacy toward BLS in the management of drowning. A strong positive correlation was found, between knowledge and attitude (r = 0.628, p = 0.001), knowledge and self-efficacy (r = 0.820, p = 0.001), and attitude and self-efficacy (r = 0.616, p = 0.001),
Supplementary Table S1 (available in online version only) presents the results of the chi-square test assessing the association between knowledge of BLS in the management of drowning and demographic characteristics. Significant associations (p < 0.05) were found between pretest knowledge scores and age, level of education, family economic status, and type of work.
Supplementary Table S2 shows the results of the chi-square test used to find the association between the attitude of BLS in the management of drowning and demographic characteristics. Significant associations (p < 0.05) were found between religion, education, type of work, and earlier attending BLS training.
Supplementary Table S3 shows the results of the chi-square test used to find the association between self-efficacy of BLS in the management of drowning and demographic characteristics. Significant associations (p < 0.05) were found between age, religion, education, family income status, and type of work.
Discussion
Drowning deaths are common in LMICs like India; timely provision of BLS is an important life-saving procedure. Learning and pursuing such training will give confidence and improve the skills, which will facilitate to save a life. Few studies were conducted to improve the hands-on skills on BLS training toward management of drowning among the public. The study found that more than three-fourths (97.8%) of the adults had not attended any BLS training in the past. These findings suggest that there is a significant gap in the knowledge and understanding of BLS among adults included in the study. The highest number of subjects (38.5%) belonged to the age group of 26 to 35 years. This has been supported by the study done in Denmark regarding sociodemographic characteristics of BLS course.17
Understanding BLS is crucial for everyone. This study focuses on to enhance the knowledge of adults who are residing in coastal areas. The present study revealed that three-fourths (80.2%) of adults had inadequate level of knowledge during pretest. Note that 45.9% adults had adequate knowledge in posttest. This results are consistent with findings reported by another study on the effectiveness of BLS training on knowledge of life-saving skills among college students in Jaipur, which showed that 79.2% participants had excellent knowledge after training.18 Study conducted with nursing students compared pre- and posttraining BLS knowledge levels and found that it significantly increased.19
The present study is also focuses on attitude to perform BLS activities. However, in real situations, positive attitude is also important in performing any activities. In this study, more than three-fourths (73.6%) of the adults had positive attitude in posttest with mean scores of 57.38 ± 6.44 in pretest and 64.87 ± 5.10 in posttest, which is similar to the other study done India.20 This finding is in agreement with the results of the study done in health care workers in Sweden21 and college students in Japan.22 A study conducted on the effectiveness of the training program on BLS techniques in Punjab showed that there was a significant difference in attitude scores at p < 0.0001.23
Additionally, the training program is to find the confidence level of adults in performance of BLS before and after training program, as described in other studies,24,25 indicating the likelihood of a practical application of the knowledge. A poor level of self-efficacy was reported among adults (58.2%) in pretest, whereas 59.3% of the adults had a fair level of self-efficacy in the posttest. Similar studies conducted with nursing students showed that following BLS training, knowledge on BLS practice, psychomotor skills, and self-efficacy significantly increased.26,27
On the other hand, a unique characteristic of the current study is to find the relationship between knowledge attitude and self-efficacy. For instance, someone with high knowledge, positive attitude, and strong self-efficacy toward BLS training program is more likely to engage in regular life-saving activity.28 The present study results showed that there is a significant correlation between knowledge and attitude (r = 0.628, p < 0.001), knowledge and self-efficacy (r = 0.820, p < 0.001), and attitude and self-efficacy (r = 0.616, p < 0.001). The findings of the previous study indicated that there is a positive relationship between BLS with knowledge and practical skills among nursing stu-dents.19 In a research with Nepalese health care professionals, Chaudhary et al found significant correlations between the dependent and independent variables.27
The association between demographic characteristics with variables in a study is crucial for understanding diversity and ensuring generalizability. In the present study, a significant association was found with knowledge and age, education, family economic status, and type of work. Similarly, attitudes and religion, education, type of work, and BLS training participation had significant association. Association is found for self-efficacy with age, religion, education, family economic status, and type of work at p < 0.05. These findings are in agreement with those of previous research from Muscat City, which found an association between knowledge levels toward BLS with gender, level of education, and occupation.11 The result was in line with the crosssectional study done in Dilla University in 2022, which showed that among variables entered into multiple logistic regression analysis departments, trained about BLS, trained advanced life support, and exposure with the person in need of BLS were significantly associated with the knowledge score.29 The present study demonstrates significant effectiveness in enhancing adults' knowledge, attitude, and selfefficacy regarding BLS in the management of drowning incidents. It confirms that BLS training programs lead to a notable increase in the number of adults capable of administering BLS to drowning victims, thereby saving lives. Furthermore, these adults can play a crucial role in disseminating BLS knowledge, both within coastal communities and throughout the broader society.
Limitations
The current study has a limitation that BLS training was carried out on mannequins, in which there will not be a real-life experience like emotion, stress, and fear that could affect the performance of CPR skills. The sample recruitment was not done on the basis of randomization, which limits the generalizability of the study results. The present study included only adult males from coastal areas. A larger or more diverse sample could have yielded different results.
Conclusion
Drowning is one of the most common accidents in the coastal region. It is best to prepare the community resources to handle emergencies as they are cost-effective and are able to respond early to emergencies. The BLS training program has been proved to be an effective strategy in improving the knowledge, attitude, and self-efficacy on the management of drowning among the general public. Initiatives such as training local communities could be carried out extensively so that lives can be saved.
Acknowledgment
We are thankful to all the participants of the study.
Ethical Approval
Ethical clearance was obtained from Yenepoya ethics committee 2, Yenepoya Deemed to university. Protocol No.YEC2/863.
Conflict of Interest
None.
References
- Accidental drowning: the importance of early measures of resuscitation for a successful outcome. Case Rep Emerg Med. 2018;2018(Jun):7525313.
- [Google Scholar]
- Fact sheet on drowning with key facts and information on the scope of the problem who is at risk prevention and WHO response. July 25, 2023. Accessed October 27, 2024 at:
- [Publisher] [Google Scholar]
- An epidemiological study of drowning survivors among school children. J Family Med Prim Care. 2017;6(04):844-847.
- [Google Scholar]
- Epidemiological profile of drowning deaths: a cross sectional study. EJFS. 2018;8(26):1-6.
- [Google Scholar]
- 83 People Died Every Day From Drowning In 2018, Yet No Prevention Plan. January 23, 2020. Accessed April 4, 2024 at
- [Publisher]
- Drowning. Rosen's Emergency Medicine; African Journal of Emergency Medicine 2011:1929-1932.
- [Google Scholar]
- Epidemiology of drowning in Bangladesh: an update. IntJ Environ Res Public Health. 2017;14(05):488.
- [Google Scholar]
- Medical conditions in scuba diving fatality victims in Australia 2001 to 2013. Diving Hyperb Med. 2020;50(02):98-104.
- [Google Scholar]
- Drowning mortality and morbidity rates in children and adolescents 0-19 yrs: a population-based study in Queensland Australia. PLoS One. 2015;10(02):e0117948.
- [Google Scholar]
- :2021.
- Fatal river drowning: the identification of research gaps through a systematic literature review. Inj Prev. 2016;22(03):202-209.
- [Google Scholar]
- Basic Life Support: Das primare ABC(D) der kardiopulmonalen Reanimation. [Basic Life Support: the primary ABC(D) of cardiopulmonary resuscitation] Ther Umsch. 1996;53(08):624-629.
- [Google Scholar]
- Evaluation of public awareness knowledge and attitudes towards basic life support among non-medical, adult population in Muscat City Oman: cross-sectional study. J Non Invasive Vasc Invest. 2020;5(02):1-8.
- [Google Scholar]
- Knowledge and attitude about basic life support and emergency medical services amongst healthcare interns in university hospitals: a cross-sectional study. Emerg Med Int. 2019;2019:9342892.
- [Google Scholar]
- Knowl?edge of first aid skills among students of a medical college in Mangalore city of South India. Ann Med Health Sci Res. 2014;4(02):162-166.
- [Google Scholar]
- Nursing students' knowledge, attitude, self-efficacy in blended learning of cardiopulmonary resuscitation: a randomized controlled trial. BMC Med Educ. 2019;19(01):414.
- [Google Scholar]
- Socio-demographic characteristics of basic life support course participants in Denmark. Resuscitation. 2022;170:167-177.
- [Google Scholar]
- A study to determine the effectiveness of basic life support training on knowledge of life saving skills among college students in selected colleges at Jaipur for degree students. IJSR. 2017;6(06):2712-2723.
- [Google Scholar]
- The effectiveness of basic life support training on nursing students' knowledge and basic life support practices: a non-randomized quasi-experimental study. Afr Health Sci. 2019;19(02):2252-2262.
- [Google Scholar]
- Basic life support: need of the hour-a study on the knowledge of basic life support among young doctors in India. Indian J Crit Care Med. 2020;24(05):332-335.
- [Google Scholar]
- The impact of CPR and AED training on healthcare professionals' self-perceived attitudes to performing resuscitation. Scand J Trauma Resusc Emerg Med. 2012;20(26):26.
- [Google Scholar]
- Factors that influence nursing staff attitudes towards initiating CPR and in using an automatic external defibrillator when outside of a hospital. Health Sci J. 2012;6:87-101.
- [Google Scholar]
- Council on Injury Violence, and Poison Prevention. Prevention of drowning. Pediatrics (05):143.:e20190850.
- [Google Scholar]
- Assessment of knowledge and self efficacy before and after teaching basic life support to schoolchildren. Rev Paul Pediatr. 2021;39:e2019143.
- [Google Scholar]
- The Effect of basic cardiopulmonary resuscitation training on cardiopulmonary resuscitation knowledge attitude, and self?efficacy of nursing students. Adv Sci Technol Letters (Healthcare and Nursing). 2015;116:56-60.
- [Google Scholar]
- Effects of two retraining strategies on nursing students' acquisition and retention of BLS/AED skills: a cluster randomised trial. Resuscitation. 2015;93:27-34.
- [Google Scholar]
- Knowledge regarding basic life support among health care workers of the hospital of Nepal. J Healthc Eng. 2023;2023:9936114.
- [Google Scholar]
- Knowledge and attitudes towards basic life support among health students at a Saudi Women's University. Sultan Qaboos Univ Med J. 2017;17(01):e59-e65.
- [Google Scholar]
- Knowledge, attitude, and practice towards basic life support among graduating class health science and medical students at Dilla University; a cross sectional study. Ann Med Surg (Lond). 2022;82:104588.
- [Google Scholar]




