

Translate this page into:
Knowledge and Practice of Dental Health among Pregnant Women in a Selected Hospital Mangaluru
Address for correspondence Pramila D'Souza, Department of OBG Nursing, Father Muller College of Nursing, Kankanady Mangaluru 575002, Karnataka, India (e-mail: dsouzapramila78@gmail.com).
This article was originally published by Thieme Medical and Scientific Publishers Pvt. Ltd. and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Introduction
Oral health is a significant part of prenatal care: health of the mouth, teeth, and gums. Pregnant mothers are more prone to cavities due to hormone surges andachangein eating habits. Although dental health is a crucial component of general health, midwives and obstetricians tend to ignore these aspects unless women complain about dental pain. This study aims to assess pregnant women's dental health knowledge and practices.
Materials and Methods
A descriptive correlational research design was adopted for the study. Atotal of 256 women were selected by using a purposive sampling technique from the antenatal wards and outpatient departments of a tertiary hospital in Mangaluru. The data were collected using the demographic proforma, structured knowledge questionnaire, and self-reported practice checklist on dental health.
Result
The mean age of the women was 27.93 ± 4.72 years. Out of the total number of women selected for the study, 56.6% were housewives, 61.7% were women from below the poverty line, and 57.8% were from rural areas. Regarding knowledge and practice, 66.4% of pregnant women had poor knowledge of dental care and 97.7% of them had an unfavorable practice of dental care during pregnancy. There was a moderate correlation between knowledge and practice of dental health during pregnancy (r = 0.038; p = 0.03).
Conclusion
The study findings show that dental care or oral health care is neglected during pregnancy.
Keywords
knowledge
practice
women
pregnancy
dental care
dental health
oral health

Introduction
Maintaining oral and dental hygiene is crucial for good periodontal health. Neglecting these practices, especially during pregnancy, can lead to infections in the mother and complications for the fetus. Despite its importance, oral hygiene often receives less attention compared with other prenatal care practices.1,2 Pregnancy induces physiological changes, including hormonal fluctuations, that increase susceptibility to gingivitis, periodontitis, and other dental issues.3,4 Research underscores the significance of diligent oral care for pregnant women, highlighting the strong connection between oral health and overall health outcomes, including the quality of life for both the mother and the developing fetus.5
A postpartum survey from the Pregnancy Risk Assessment Monitoring System, conducted across 10 states, revealed that 56% of mothers did not consider dental checkups, and 60% did not have their teeth cleaned routinely during pregnancy.6 Additionally, a report from 2007 to 2009 indicated that 56% of pregnant women did not visit a dentist.7 A cohort study of pregnant women in Hyderabad, South India, also showed inadequate knowledge regarding oral health.8 Despite facing oral health issues during pregnancy, many women avoid dental examinations.9 This avoidance is often infl uenced by socioeconomic and cultural factors, as well as myths, such as the belief that dental examinations are unsafe during pregnancy.10 Social media and health care professional counseling can improve knowledge in both urban and rural areas. However, limited awareness, concerns about dental costs, lack of referral processes, and certain rituals and customs during pregnancy continue to contribute to poor dental care practices.11 This neglect can adversely affect the oral health of women during and after pregnancy. Moreover, untreated dental problems in mothers can pose a risk of transmitting bacteria to the child during lactation.10,12
The World Health Organization (WHO) advocates for a preventive approach that emphasizes timely, comprehensive, and inclusive care rather than a curative one.13 The available literature indicate that assessing a woman's oral health at the first prenatal visit and conducting monthly follow-ups can help protect both the mother and the fetus. Therefore, the investigators aimed to understand the awareness and compliance of expectant mothers regarding dental health checkups.
Materials and Methods
A descriptive correlational research design was adopted to identify the knowledge and self-reported practices of dental health in pregnant women. The study also corelated knowledge and practice of dental health among pregnant women and the association between the knowledge and practice with selected demographic variables.
The purposive sampling technique was used to select 256 pregnant women who visited the antenatal outpatient department and those admitted to a tertiary hospital for safe confinement. All pregnant women after 38 weeks of gestation and women who were available during data collection were included in the study. Those women who cannot read and write Kannada and English and women with systemic disorders like diabetes and progressive diseases of the mouth were excluded from the study. The sample size was calculated with a confidence level of 95%, a margin of error of 5%, and a population proportion of 80%.
The below-mentioned formula is used to calculate the sample size:
Total sample size taken for the study was 256.
Data Collection Instrument
The instruments used were the following: socioeconomic proforma, a knowledge questionnaire consisting of 16 questions on dental health, and a self-reported practice checklist. It covered three areas: dental problems, causes of tooth decay, and prevention and management. The pregnant women were instructed to put a tick mark against the most suitable answer. Each correct answer was scored “1” and each incorrect answer was given a score of “0.” A maximum score of 16 was arbitrarily assigned to poor (>5), average (6–10), and good (1 and above). The self-reported checklist contained 10 questions with yes/no answers. Each correct answer was scored “1” and each wrong answer was given a score of “0.”
Reliability of the subject was performed among 20 pregnant women The reliability was found using the Karl Pearson correlation coefficient and the tool was found reliable (0.87).
Data Collection Process
The main study was conducted from March 2 to April 30,2021. After the ethical clearance (FMIEC/CCM/236/2020), formal permission was obtained from the concerned authority before data collection. Participants who fulfilled the sampling criteria were identified. The researchers introduced themselves and explained the purpose to the participants. The participant sheet was explained and written consent was obtained from the participants. The demographic proforma was collected through an interview technique, knowledge was assessed using the structured knowledge questionnaire, and a selfreported practice checklist was filled by the participants.
Data collected were compiled for analysis. The data were analyzed using SPSS version 23.
Results
A total of 38.3% of pregnant women with a mean age of 27.93 years were in the age group of 26 to 30 years. About 35.2% of women had higher education or a degree, 56.6% were homemakers, 57.8% lived in rural areas, and 61.7% women were from below-poverty-line (BPL) families. Regarding dental health, 66.4% had poor knowledge, 30.9% had average knowledge, and only 2.7% had good knowledge. While 56% were aware of the causes of dental problems, 38.6% understood prevention and management. However, 97.7% had an unfavorable dental practice, with only 2.3% having a favorable practice. There was no significant association between demographic variables and practice (p > 0.05) or knowledge (p > 0.05), as shown in Table 1 and 2. Fig. 1 indicates a weak positive correlation between knowledge and practice (r = 0.38; p = 0.547).
| Sl. no. | Baseline variables | <Median (≤4) | >Median (≥5) | χ2 | Df | p value |
|---|---|---|---|---|---|---|
| 1 | Age (y) | |||||
| 20–25 | 36 | 47 | 0.283 | 2 | 0.868 | |
| 26–30 | 39 | 59 | ||||
| 31–35 | 30 | 45 | ||||
| 2 | Occupation | |||||
| Employed | 53 | 58 | 3.671 | 1 | 0.072 | |
| Homemaker | 52 | 93 | ||||
| 3 | Qualification | |||||
| Primary | 18 | 17 | 6.080 | 3 | 0.108 | |
| SSLC | 32 | 34 | ||||
| PUC | 20 | 45 | ||||
| Degree and above | 35 | 55 | ||||
| 4 | Economic status | |||||
| APL | 37 | 61 | 0.698 | 1 | 0.435 | |
| BPL | 68 | 90 | ||||
| 5 | Residence | |||||
| Urban | 41 | 67 | 1 | 0.720 | 0.441 | |
| Rural | 64 | 84 | ||||
Abbreviations: APL, above poverty line; BPL, below poverty line; PUC, preuniversity course; SSLC, secondary school leaving certificate.
| Sl. no. | Baseline variables | <Median (≤4) | >Median (≥5) | χ2 | Df | p value |
|---|---|---|---|---|---|---|
| 1 | Age (y) | |||||
| 20–25 | 33 | 50 | 4.724 | 2 | 0.94 | |
| 26–30 | 37 | 61 | ||||
| 31–35 | 40 | 35 | ||||
| 2 | Occupation | |||||
| Employed | 51 | 60 | 0.709 | 1 | 0.237 | |
| Home maker | 59 | 86 | ||||
| 3 | Educational Qualification | |||||
| Primary | 22 | 13 | 7.854 | 3 | 0.445 | |
| SSLC | 27 | 39 | ||||
| PUC | 29 | 36 | ||||
| Degree and above | 32 | 58 | ||||
| 4 | Economic status | |||||
| APL | 42 | 56 | 0.001 | 1 | 0.977 | |
| BPL | 68 | 90 | ||||
| 5 | Residence | |||||
| Urban | 45 | 63 | 0.129 | 1 | 0.798 | |
| Rural | 65 | 83 | ||||
Abbreviations: APL, above poverty line; BPL, below poverty line; PUC, preuniversity course; SSLC, secondary school leaving certificate.
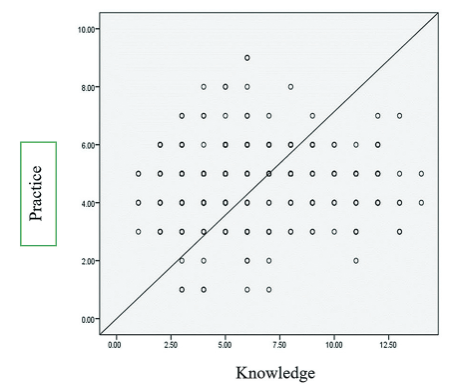
- Relationship between knowledge and practice of dental health among pregnant women.
Discussion
Research studies have been conducted across various countries with regard to knowledge and practice about women's oral health during pregnancy. Research connects oral health care to overall health, pregnancy outcomes, and the health of the unborn child. In the present study, most participants aged over 30 years, including primi mothers, had attained higher education. These findings align with a study by Hosseini et al who stated that the majority of the women who visited the Perinatal Clinic in Iran were aged between 17 and 38 years and had tertiary education.14 Chinenye-Julius et al reported in their study that the majority of the respondents, that is, approximately 51.9%, were between the ages of 25 and 34 years.15
The current study concluded that the participants had insufficient knowledge and practice about dental health. A similar research study from Nigeria reported low knowledge of oral hygiene and poor compliance to oral hygiene practices.15 In addition, Daneshvar et al reported moderate knowledge during pregnancy.16 Also, an institution-based survey conducted by Wassihun et al17 and Hu et al18 included approximately 224 women and reported a lack of dental care during pregnancy. These results are consistent with the results of the present study. Overall, comparing these studies, it has been found that the majority of the participants lack oral hygiene and are unaware of the various dental health practices due to unfavorable beliefs about safety issue of dental procedures and reluctance on assessing oral health.19,20
On the other hand, Javali et al21 identified good understanding and attitude toward oral hygiene among expectant mothers, but its practices were limited. Barbosa et al22 found that mothers had sufficient knowledge of oral health during pregnancy and childbirth. A couple of studies explain that oral health is one of the essential components of assessment that should not be neglected throughout pregnancy.19,23,24 Although the obstetrician and midwives are aware of it, there is a tendency to neglect it unless a woman has complaints of tooth ache. In the present study, women showed poor knowledge and practice, which could be due to limited awareness or lack of referrals provided during antenatal visit. Hence, the study highlights a need for protocols for continuing education, training, and referral of pregnant women from health centers.
In regard to knowledge and practice, the study highlights a moderate correlation between knowledge and practice. Researchers have observed a connection between high birth weight, frequent brushing, and frequency of oral cavity issues and dental treatment during pregnancy.13,25 Also, the findings of a study done by Wassihun et al17 and Daneshvar et al16 reported the relationship of knowledge and selected baseline variables. In addition, most studies have linked oral health knowledge to education, income, occupation, health care access, myths, and prenatal counseling.12,20 However, the present study showed contradicting results. No significant association was found between demographic variables and knowledge or practice.
Conclusion
The outcomes of the current study highlight the need for integrated education on dental health through various health promotion interventions. Consistent visits to a dentist, practicing good oral hygiene throughout life, and awareness of the safety and significance of dental health during pregnancy can improve the overall health and wellbeing of women. Thus, this study underscores the importance of preventive and primary oral treatment for pregnant women.
Conflict of Interest
None declared.
References
- A questionnaire-based survey to assess the knowledge and awareness of denture staining in complete denture wearers. J Health Allied Sci NU. 2019;9(02):45-50.
- [Google Scholar]
- Pregnant women's perspectives on integrating preventive oral health in prenatal care. BMC Pregnancy Childbirth. 2021;21(01):271.
- [Google Scholar]
- Poor oral health-related quality of life among pregnant women: a systematic review and meta-analysis. Int J Dent Hyg. 2021;19(01):39-49.
- [Google Scholar]
- Assessment of oral health status during pregnancy. Natl J Physiol Pharm Pharmacol. 2021;11(08):806-809.
- [Google Scholar]
- The impact of pregnancy on women's oral health-related quality of life: a qualitative investigation. BMC Oral Health. 2020;20(01):294.
- [Google Scholar]
- Disparities in access to oral health care. Annu Rev Public Health. 2020;41:513-535.
- [Google Scholar]
- Pregnancy, oral health and dental education: an overview on the northeast of Italy. J Perinat Med. 2020;48(08):829-835.
- [Google Scholar]
- Oral health knowledge among a cohort of pregnant women in south India: a questionnaire survey. J Family Med Prim Care. 2020;9(06):3015-3019.
- [Google Scholar]
- Stressful life events oral health to barriers dental care during pregnancy. J Public Health Dent. 2023;83(03):275-283.
- [Google Scholar]
- Factors influencing the provision of oral health care practices by antenatal care providers: a systematic review. J Womens Health (Larchmt). 2022;31(02):231-241.
- [Google Scholar]
- Knowledge and attitudes on oral health of women during pregnancy and their children: an online survey. BMC Oral Health. 2024;24(01):85.
- [Google Scholar]
- How much do pregnant women know about the importance of oral health in pregnancy? Questionnaire-based survey. BMC Pregnancy Childbirth. 2023;23(01):348.
- [Google Scholar]
- Oral and health dental status of pregnant women referred to perinatal clinics in southeastern Iran. J Res Dent Maxillofac Sci. 2023;8(02):79-87.
- [Google Scholar]
- Knowledge, attitude and practices of oral hygiene among pregnant women attending antenatal clinics in Nigeria: evidence from Ogun state. Afr J Health Sci. 2021;34(01):44-54.
- [Google Scholar]
- Oral health among pregnant women at Ilam, Iran: a KAP study. J Health Rep Technol. 2023;9(02):1-4.
- [Google Scholar]
- Knowledge of oral health during pregnancy and associated factors among pregnant mothers attending antenatal care at South Omo Zone public hospitals, Southern Ethiopia 2021. PLoS One. 2022;17(08):e0273795.
- [Google Scholar]
- Oral health status and literacy/knowledge amongst pregnant women in Shanghai. Int Dent J. 2023;73(02):212-218.
- [Google Scholar]
- Dental care during pregnancy based on the pregnancy risk assessment monitoring system in Utah. BMC Oral Health. 2019;19(01):237.
- [Google Scholar]
- The role of oral and prenatal healthcare providers in the promotion of oral health for pregnant women. BMC Pregnancy Childbirth. 2023;23(01):313.
- [Google Scholar]
- Oral health knowledge, attitude, and practice of pregnant women in Deccan, South India: a cross-sectional prenatal survey. J Med Life. 2022;15(03):420-424.
- [Google Scholar]
- Maternal knowledge of oral health during pregnancy and childbirth. Matern Child Health J. 2023;27(09):1607-1615.
- [Google Scholar]
- Perceptions, knowledge, and practices related to oral health in a group of pregnant women: a qualitative study. Clin Exp Dent Res. 2024;10(01):e823.
- [Google Scholar]
- Knowledge, attitude, and practice towards oral health among pregnant women attending antenatal care at Siriraj Hospital. Thai J Obstet Gynaecol. 2023;31(03):182-191.
- [Google Scholar]
- Unfavourable beliefs about oral health and safety of dental care during pregnancy: a systematic review. BMC Oral Health. 2023;23(01):762.
- [Google Scholar]




